
Summary
Proteins are essential for our body and have many functions. They act as messengers, help with cell structure, control chemical reactions, transport oxygen, and provide energy. Different parts of our body, such as bones, muscles, and tendons, contain proteins. Our body continuously breaks down and builds new proteins every day. Proteins are made up of smaller units called amino acids. Twenty different amino acids make up all the proteins in our body. When we eat protein-rich foods, our body uses the amino acids from those proteins to build new proteins or provide energy. If we do not get enough essential amino acids from our diet, our body may break down muscle proteins for energy.
The kidneys play a crucial role in the processing of proteins. They filter blood and remove waste proteins such as ammonia, urea, and creatine, which are produced when proteins are broken down. The Glomerular Filtration Rate (GFR) and creatinine tests are used to evaluate kidney function. GFR measures how well the kidneys filter blood, while creatinine levels indicate how much muscle protein waste is created and excreted by the kidneys. Abnormal levels of creatinine and decreased GFR can be signs of kidney dysfunction or chronic kidney disease. Factors like diet, hydration, muscle mass, and certain medications can affect creatinine and GFR levels.
Maintaining a balanced diet, including plant-based proteins rich in essential amino acids, proper hydration, and a healthy microbiome, is vital for protein synthesis and kidney health. Chronic kidney disease can have serious consequences, so early recognition and appropriate management are essential to prevent complications.
What is eGFR and Creatinine?
The Complete Metabolic Panel (CMP) includes the estimated Glomerular Filtration Rate (eGFR) and creatinine (Cr) tests. The eGFR test estimates how much blood passes through the glomeruli, the tiny filters in the kidneys, each minute. The Cr test measures muscle protein breakdown and filtration through the kidneys.
Why does eGFR and Creatinine Matter?
eGFR and creatinine assess protein metabolism and kidney function.
Much of the body is made of protein, and these proteins take on a myriad of forms and functions. They represent cell signaling receptors, signaling molecules, structural members, enzymes, intracellular trafficking components, extracellular matrix scaffolds, ion pumps, ion channels, oxygen and CO transporters (hemoglobin). Protein is in bones (collagen), muscles (creatine), and tendons; the hemoglobin that transports oxygen; and enzymes that catalyze all biochemical reactions. Protein is also used for growth and repair, communicating between receptors and molecules, and makes up part of the cell structure. Amid all these necessary functions, proteins also serve as an energy source.
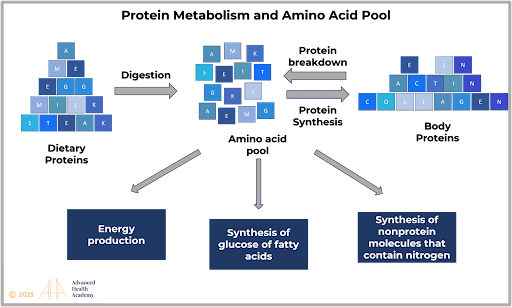
Every day over 250 grams of protein in your body are dismantled, and 250 grams of new protein are built. Proteins are long chains of amino acids that are connected to one another by peptide bonds. An amino acid contains an amino (-NH2) and carboxylic acid (-COOH) functional group, hence the amino acid. Proteins are unique based on which amino acids they contain, how they are arranged in a chain, and the complex interactions the chain makes with itself and the environment [14][15].

Proteins are not stored for later use, so excess proteins must be converted into glucose (glycogen in muscle and liver) and lipids (as triglycerides in fat tissue) and used to supply energy or build energy reserves. To form new proteins, amino acids derived from food and muscle protein metabolism are placed into a “pool.” Because more than 90 percent of the protein ingested does not get broken down further than to amino acids, it is critical to continuously replenish the cellular “pool” with proteins rich in essential amino acids. Otherwise, the body must break down muscle protein as an energy source.
Although hundreds of amino acids are found in nature, only about 20 make all the proteins found in the human body and most other forms of life. They include:
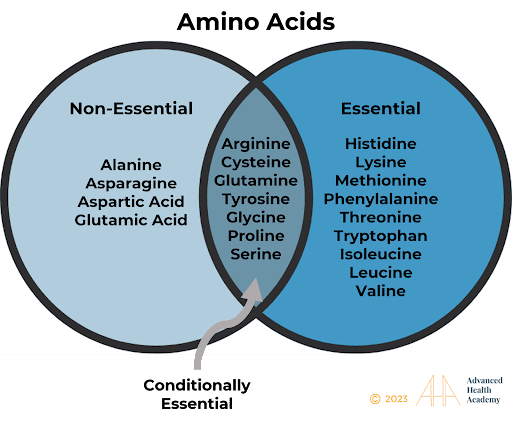
Essential amino acids must be present for humans and other mammals to synthesize all 20 amino acids [17],[18]. Non-essential amino acids cannot be used to make protein.
Protein Metabolism
The digestion of protein derived from food begins in the stomach. The enzyme pepsin and hydrochloric acid (HCl; 0.5 percent) produces a pH of 1.5–3.5 that denatures proteins into smaller polypeptides and their constituent amino acids. This food-gastric juice mixture (chyme) then enters the small intestine, where the bacteria plays the most significant role in releasing enzymes, including secretin and cholecystokinin (CCK), critical for breaking apart proteins into individual amino acids. The bacteria also metabolize vitamins and ferment indigestible carbohydrates (plant-derived dietary fiber) to short-chain fatty acids (e.g., acetate, propionate, butyrate). Secretin stimulates the pancreas to release sodium bicarbonate and most of the digestive enzymes, including the proteases trypsin, chymotrypsin, and elastase, which aid protein digestion and neutralize the HCl (essential for protecting the intestines’ lining). Individual amino acids are then transported across the small intestines, mediated by sodium-amino acid transporters, and into the bloodstream to be transported to the liver and cells throughout the body.
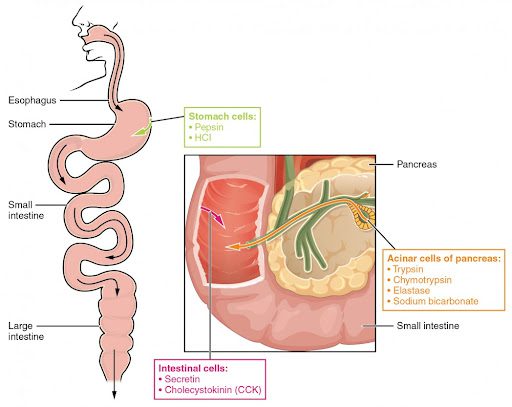
Enzymes in the stomach and small intestine break down proteins into amino acids. HCl in the stomach aids in proteolysis, and hormones secreted by intestinal cells direct the digestive processes.
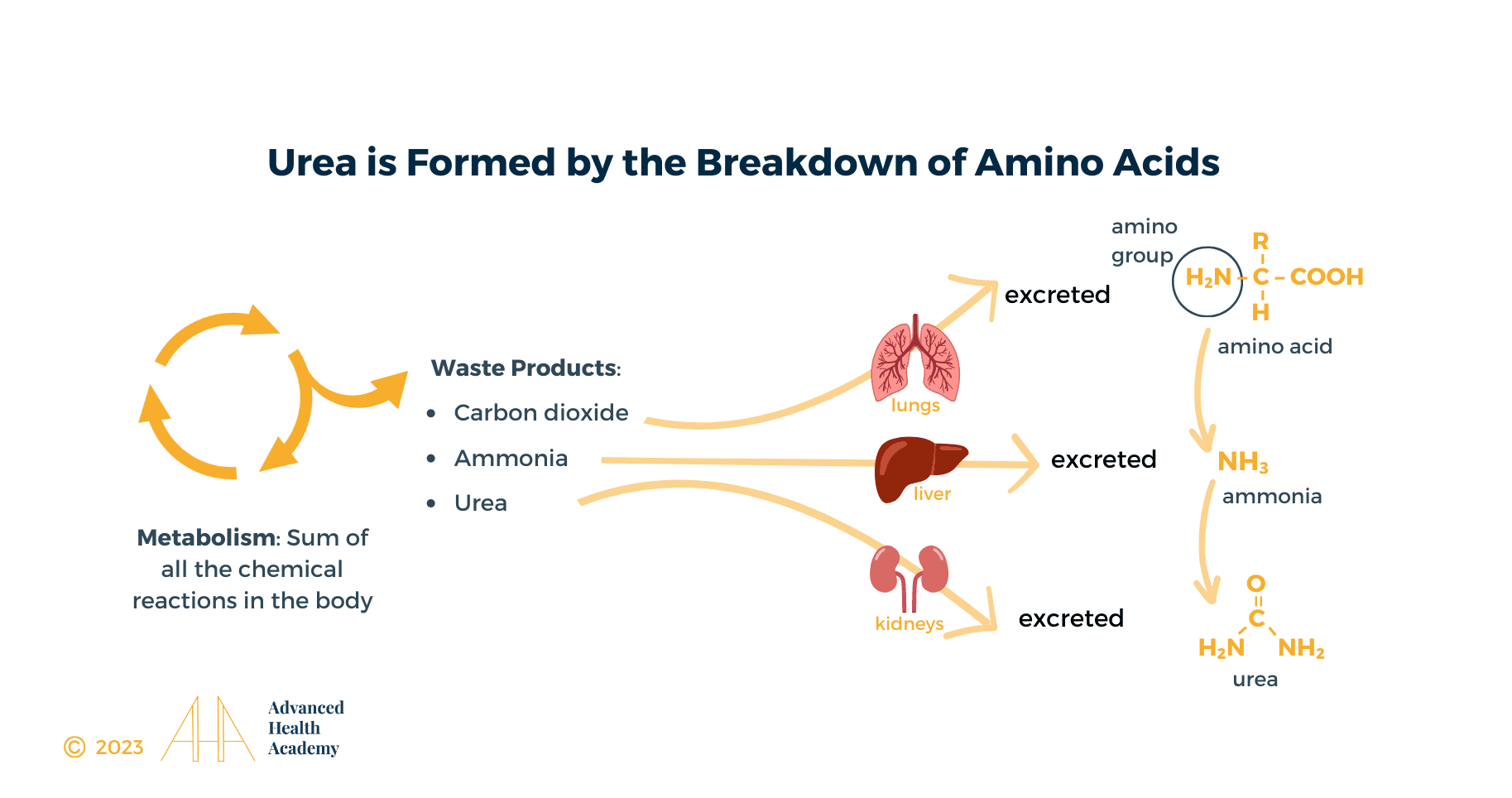
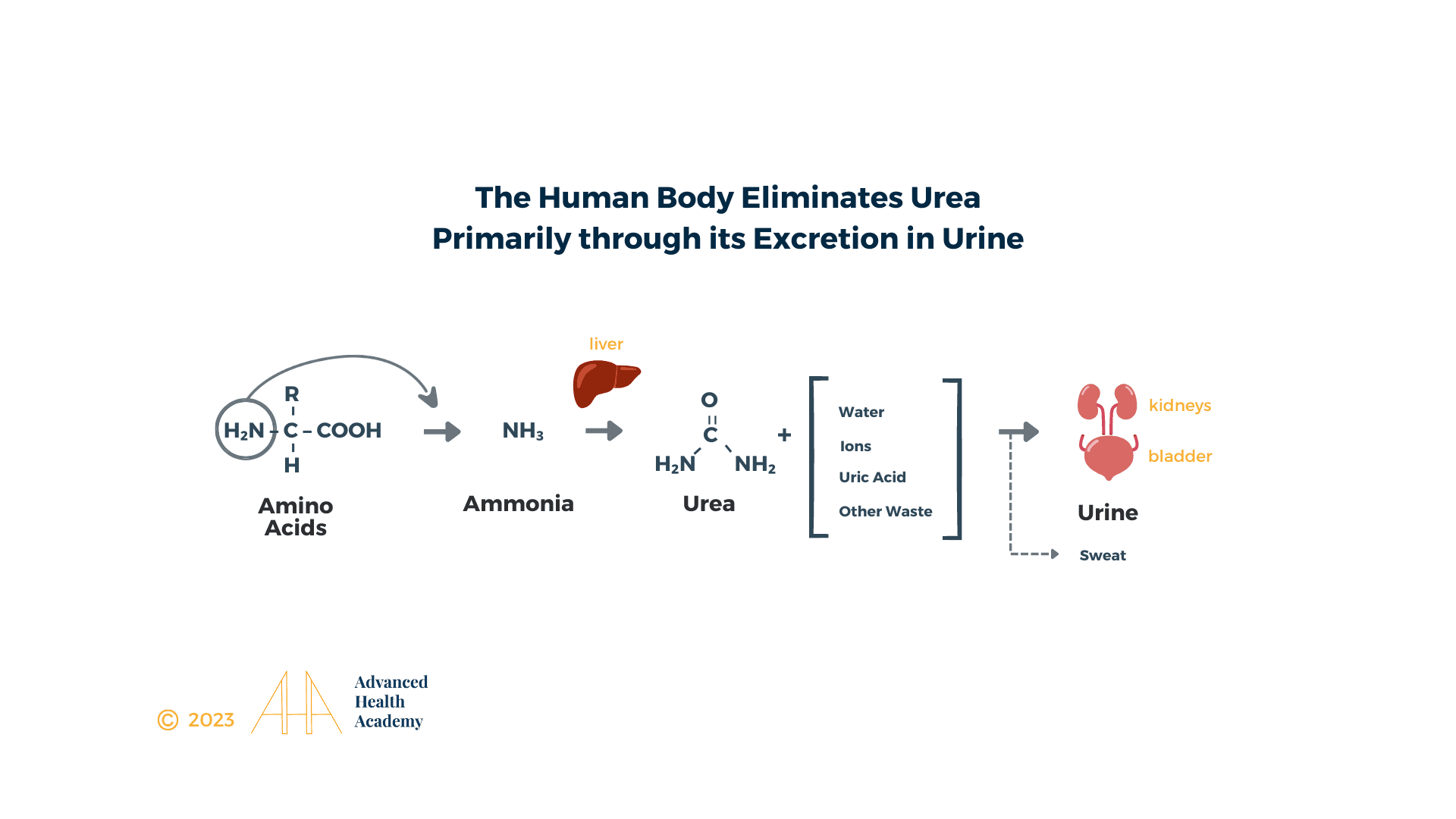
Urea Cycle
The processing of amino acids results in the creation of metabolic intermediates, including pyruvate, acetyl CoA, acetoacetyl CoA, oxaloacetate, and α-ketoglutarate, which are used as energy sources via the Krebs cycle; hydrocarbons, and toxic toxic amino groups (-NH2). NH2 is degraded in the liver to ammonia (NH3) and then converted to less toxic urea, carbon dioxide (CO2), and water. Urea is released into the bloodstream and transported to the kidneys, with 40-50% appearing in urine. Sweat, stool, and exhalation eliminate less than 10% of urea. The remaining 40-50% of urea is stored as fat in the liver, abdominal cavity, and muscle tissue or accumulates in the blood.
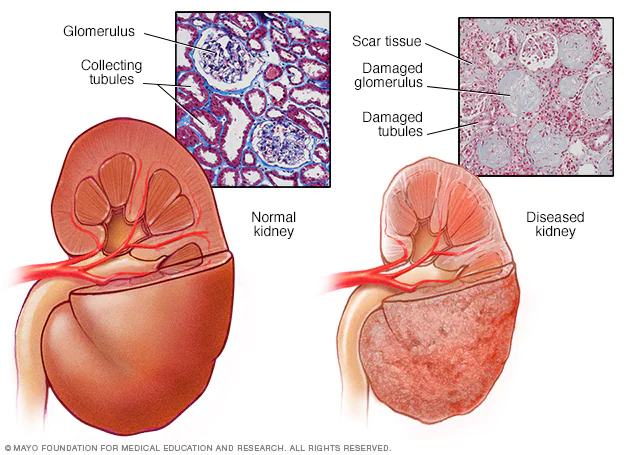
The kidneys are two bean-shaped organs, each about the size of a fist, located just below the rib cage, one on each side of your spine. Healthy kidneys filter about a half cup of blood every minute, equivalent to about 150 quarts of blood.
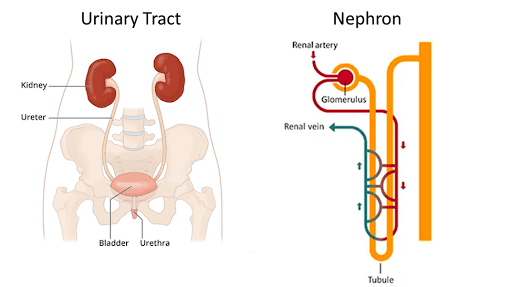
Each kidney has millions of nephrons of small blood-filtering units called the glomerulus and a tubule. The kidneys maintain a healthy balance of water, proteins, salts, and minerals – such as sodium, calcium, phosphorus, and potassium – in the blood, essential for every organ to function, and excrete 1 to 2 quarts of excess water, ions, cellular and protein waste in the form of urine. The kidneys also make hormones that help control blood pressure, make mature red blood cells, and keep bones strong.
The urine flows from the kidneys to the bladder through two thin tubes of muscle called ureters, one on each side of your bladder. Urine is stored in the bladder and removed during urination.
Why Does Abnormal GFR and Creatinine Matter?
An abnormal creatinine level is influenced by the protein content of diet and any pathology associated with the breakdown of muscle protein and the consequent increased excretion of protein waste products such as uric acid, urea, creatinine, and cystatin C, and other impurities by the kidneys [16].
Normal Range
The normal creatinine values may vary among laboratories, ethnicities, age, and gender. Children produce less urine than adults, and the amount produced depends on their age.
A “normal” serum creatinine level does not necessarily mean the kidney function is normal. Serum creatinine is influenced by physiologic variables such as muscle mass (age-dependent, lower in women, higher in African-Americans) and diet (lower in vegans, higher with ingestion of cooked meats).[3]
According to the National Kidney Foundation[1], the current normal serum creatinine range is:
- Men aged 18-60: 0.9–1.3 mg/dL
- Men age 60+: 0.8–1.3 mg/dL
- Women aged 18-60: 0.6–1.1 mg/dL
- Women age 60+: 0.6–1.2 mg/dL
GFR is a more precise estimation of kidney function where disease severity correlates closely but inversely with GFR. GFR is calculated with the following inputs: Blood/serum Creatinine level (mg/dL), age (years), sex, and ethnicity (Black Americans versus not).
GFR = 175 × (serum creatinine in mg/dL)-1.154 × (age)-0.203 × (0.742 if female) × (1.212 if Black)
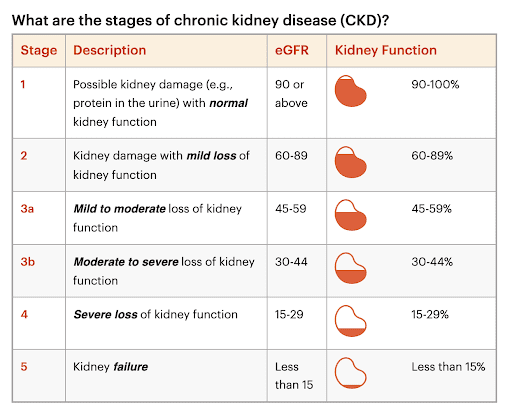
The normal GFR is 125 mL/min/1.73 m2, presumptively showing healthy, functioning kidneys. Older people will have lower than normal GFR levels because GFR decreases with age. There are five stages of chronic kidney disease (CKD) starting with GFR < 90 mL/min for 3 or more months[2][4][5]:
- Stage 1 with normal or high GFR (GFR > 90 mL/min)
- Stage 2 Mild CKD (GFR = 60-89 mL/min)
- Stage 3A Moderate CKD (GFR = 45-59 mL/min)
- Stage 3B Moderate CKD (GFR = 30-44 mL/min)
- Stage 4 Severe CKD (GFR = 15-29 mL/min)
- Stage 5 End Stage CKD (GFR <15 mL/min) = kidney failure where dialysis needs to be considered.
Optimal Range
The most up-to-date medical research shows that the optimal range of creatinine and eGFR is a half standard deviation from the lab mean in certain specific ethnicities.
High Creatinine and Decreased GFR Levels
When creatinine levels are higher than normal and GFR is decreased, it is typically a sign of kidney dysfunction or chronic kidney disease (CKD).
An elevated creatinine level is caused by increased muscle protein metabolism due to insufficient consumption of proteins rich in essential amino acids, critical for protein synthesis. The number one cause is a high animal-protein diet.
Animal proteins like dairy products, poultry, eggs, red meat, and fish contain non-essential amino acids. They require more digestive juices, water, and abundant healthy gut bacteria to be processed than plant-based proteins rich in essential amino acids. Adding 10 percent saturated fat (primarily from animal sources) increases the conversion of animal proteins into nitrosamines, toxic byproducts that must be filtered and excreted by the kidneys. Elevated nitrosamines in the blood accelerate cell death and gene mutation, altering gene expression and organ function throughout the body. Animal protein consumption increases the risk of chronic kidney disease, cancer, infection, autoimmune disorders, and other preventable chronic physical and mental illnesses by 44%.
The other leading causes of a high total creatinine level and low GFR are 1) increased tissue damage, e.g., malnutrition, trauma, major surgery, severe infection, strenuous exercise, and certain drugs; and 2) low circulatory states, e.g., severe gastrointestinal bleed, heart failure [9], severe dehydration [10], substantial blood loss, and hypovolemic shock. They all induce a catabolic state with increased muscle protein (creatine) breakdown and consequent increase in blood creatinine without necessarily changing the GFR. Another culprit is a complete or partial blockage of urine flow in the kidneys, ureters, bladder, and urethra, which increases the risk of kidney damage, kidney stones, and infection.
The most widely cited drug group for elevated serum creatinine levels are antibiotics such as trimethoprim-sulfamethoxazole (Bactrim/Septra), cephalexin (Keflex), cefuroxime (Ceftin), cefaclor (Ceclor), aminoglycosides such as gentamicin, tobramycin, amikacin, plazomicin, streptomycin, neomycin, and paromomycin; corticosteroids such as cortisone, hydrocortisone, and prednisone; non-steroidal anti-inflammatories (e.g., Ibuprofen, Naproxen, Aloxiprin); antacids such as H2 blocker Cimetidine (Tagamet, Famotidine (Pepcid), and Ranitidine (Zantac); cholesterol medications such as Fenofibrate (Tricor), Pyrimethamine (a medication to treat parasites), anti-seizure medication such as Phenacemide to name a few.[7][8][11][12]
Suppose the root cause is not adequately addressed. In that case, the kidneys struggle to balance electrolytes, blood and urine acidity, alkalinity and fluid levels, and blood pressure and make mature red blood cells. Other organ functions are also negatively impacted. For example, the liver struggles with detoxifying the blood, balancing hormone levels, cholesterol metabolism, and many other essential functions. The digestive system struggles to break down food, absorb essential nutrients, and produce nitric oxide, which is critical for making energy and for every organ in the body to function correctly. This inevitably leads to poorly digested cholesterol depositing on the inside lining of blood vessels, triggering an inflammatory response and restricting blood flow throughout the body.
Chronic kidney disease (CKD) is a widespread public health problem with substantial morbidity and mortality. Recognizing CKD in its early stages and preventing its worsening and associated complications is critical. CKD-associated outcomes are difficult-to-treat hypertension, kidney stones, kidney failure, cardiovascular disease, and premature death.[6]
Low Creatinine and Decreased GFR Levels
When creatinine levels are lower than the normal range, and GFR is decreased, it can indicate any of the following:
1) A low animal protein diet and sufficient consumption of essential amino acids derived from plant-based whole foods
2) More commonly, kidney dysfunction or CKD due to the following causes:
- Inadequate blood flow to the kidneys or excess loss of body fluids
- Damage to the glomeruli and/or tubules of the kidneys
- Obstruction of urine flow within any part of the urinary tract.
3) A person with low muscle mass or body weight
4) Malnutrition
5) Chronic dehydration, insufficient hydrochloric acid and digestive enzymes, or dysbiosis (deficient healthy bacteria in the gut relative to pathogenic bacteria) – all essential for protein metabolism.
6) Elevated cortisol production and an overstimulated sympathetic nervous system cause suppression of many organ functions, elevate inflammation, and increase muscle protein metabolism.
Sources:
- Normal creatinine lab minimum and maximum: Quest Diagnostics – Creatinine
- Estimated Glomerular Filtration Rate (eGFR). National Kidney Foundation. https://www.kidney.org/atoz/content/gfr. Published December 24, 2015. Accessed June 8, 2023.
- https://www.niddk.nih.gov/health-information/kidney-disease/kidneys-how-they-work#:~:text=Your%20kidneys%20remove%20wastes%20and,and%20potassium%E2%80%94in%20your%20blood
- A steady increase in mortality was predicted for Medicare patients (aged > or = 65 years) who were hospitalized for myocardial infarction (n = 44,437) who had increased levels of BUN > 17 mg/dL(> 6.1 mmol/L), creatinine > 1.0 mg/dL (> 88.4 micromol/L), and eGFR < 100 mL/min per 1.73 m2 and in patients who experienced heart failure who had increased levels of BUN > 16 mg/dL (> 5.7 mmol/L), creatinine > 1.1 mg/dL (> 97.2 micromol/L), and a Mayo eGFR <= 90 mL/min per 1.73 m2. Gotsman I, Zwas D, Planer D, Admon D, Lotan C, Keren A. The significance of serum urea and renal function in patients with heart failure. Medicine (Baltimore). 2010;89(4):197-203. [PubMed]
- “In our experience with athletes, we frequently observed high creatinine values, near or higher than 115 μmol/L (1.3 mg/dL).” Banfi G, Del Fabbro M. Serum creatinine values in elite athletes competing in 8 different sports: comparison with sedentary people. Clin Chem. 2006;52(2):330-331. [PubMed]
- Levey AS, Eckardt KU, Tsukamoto Y, et al. Definition and classification of chronic kidney disease: a position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2005;67(6):2089-2100 [PubMed] [Google Scholar]
- Stevens L, Perrone RD.Drugs that elevate the serum creatinine concentration UpToDate Online. http://uptodateonline.com/online/content/topic.do?topicKey=fldlytes/32725&selectedTitle=2~150&source=search_result Accessed December 17, 2008.
- Warren GV, Korbet SM, Schwartz MM, Lewis EJ. Minimal change glomerulopathy associated with nonsteroidal antiinflammatory drugs. Am J Kidney Dis. 1989February;13(2):127-130 [PubMed] [Google Scholar]
- Aronson D et tal. Elevated blood urea nitrogen level as a predictor of mortality in patients admitted for decompensated heart failure. The Am J Med 2004; 116, 7: 466-73.
- Mehta AR. Why does the plasma urea concentration increase in acute dehydration? Advances in physiology education 2008; 32, 4: 336.
- Andreev, E., et al. (2001). A rise in plasma creatinine that is not a sign of renal failure: Which drugs can be responsible? Journal of International Medicine.
- Berg, K. J., et al. (1989). Renal effects of trimethoprim in ciclosporin- and azathioprine-treated kidney-allografted patients. Nephron.
- LaPelusa A, Kaushik R. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Nov 14, 2022. Physiology, Proteins.
- Benjamin O, Lappin SL. StatPearls [Internet]. StatPearls Publishing; Treasure Island (FL): Jul 19, 2022. Kwashiorkor
- ROSE WC. The amino acid requirements of an adult man. Nutr Abstr Rev. 1957 Jul;27(3):631-47.
- Watford M. The urea cycle: Teaching intermediary metabolism in a physiological setting. Biochem Mol Biol Educ 2003; 31, 5: 289-97.
- Wu G. Amino acids: metabolism, functions, and nutrition. Amino Acids. 2009 May;37(1):1-17.
- de Koning TJ. Amino acid synthesis deficiencies. Handb Clin Neurol. 2013;113:1775-83.